Ankle Sprains
Treatment administered in the first 24 hours is the most important determinant of long-term recovery from an acute ankle sprain. Chronic or recurrent ankle sprains also need physiotherapy rehabilitation to achieve stability and should be treated immediately by one of our physiotherapists to improve stability and decrease pain.
Presentation
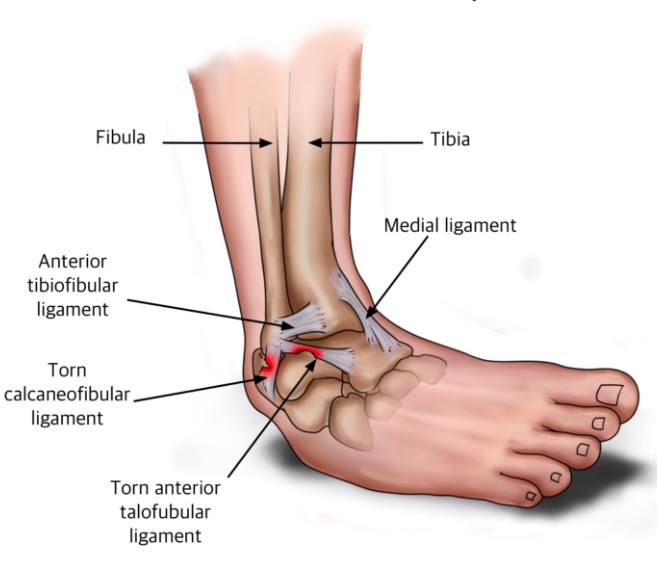
The most common type of ankle sprain is due to excessive inversion and plantarflexion, called an “inversion sprain”, and stretches or tears the lateral and anterior ankle ligaments, can damage the retinaculum and often impinges the medial ankle structures. Egg-shaped swelling appears on the outside of the ankle. A grade one injury is caused by mild over-stretching with less than 10% of ligament fibres torn. A grade two injury involves considerable tearing of the ligament fibres and a grade three injury is a complete rupture or avulsion of a ligament.
Treatment
Contact our physios at Rivervale Physiotherapy for treatment within the first 24-72 hours aiming to preventing further damage and reducing swelling by immobilising the ankle in an everted and dorsiflexed position. This can be effectively achieved by rigid strapping with compression that can be loosened by the patient if the ankle continues to swell. Keeping the ankle elevated above the level of the heart and applying icepacks to the ankle for 20-30 minutes every 2 hours is effective at reducing pain and swelling also. If the injury is a grade 2 or 3 sprain, the patient should use crutches for the first 48-72 hours and partial weight bearing should commence after this time to assist with removal of oedema. Early but gentle active and passive mobilisations to the subtalar and talo-crural joints have been shown to recover range of movement safely and effectively. Treatment in the sub-acute phase consists primarily of exercises and manual therapy to regain proprioception, strength and range of movement.
Chronic or Recurrent Ankle Sprains
Recurrent ankle injuries are unfortunately far too common and the two main factors leading to recurrent or chronic injuries are poor proprioception and stiffness of the talocrural joint, where most of the ankle’s eversion and inversion movement occurs. Proprioceptive retraining, or balance retraining, should commence as soon as practical following an acute ankle injury and exercises should be continued for at least 8 weeks post-injury. If proprioception is not retrained, the patient will be at high risk of recurrence and can eventually develop chronic ankle weakness and instability. It can take up to 9 months for the ankle to regain full strength and balance following a moderate injury.
Avulsion or Talar Dome Fractures
Severe swelling and bruising following acute injury can indicate either an avulsion fracture or a talar dome fracture. An X-ray will determine the presence of a ligamentous avulsion fracture, but the talar dome fracture (cartilaginous) will not show up on plain X-ray. If the ankle does not respond to conservative management as expected, or if the ankle remains unstable with weight bearing, a talar dome fracture should be suspected and a bone scan or CT scan arranged. Large talar dome fractures usually require surgery, with MACI (chondral grafting) now showing excellent results for these cartilaginous lesions.
Fracture of 5th Metatarsal
A fracture of the head of the 5th metatarsal is also possible with an inversion ankle injury. These injuries can be easily missed, as the patient can be fully weight bearing with only moderate discomfort. More pronounced swelling and bruising extending into the lateral foot is usually observed in these cases.
Contact us at Rivervale Physiotherapy for treatment or further information.